
















 18 / 72
18 / 72

16
disabilities are abandoned and are consequently
cared for by institutions, which are detrimental to
their development and carry significant and long-term
costs for the state. By integrating the early interven-
tion programme into the health and social systems,
the number of abandoned children can be significant-
ly reduced. This development model helps children
to achieve better results, protects their human rights,
supports families, and saves precious resources for
the community.
THE MODEL:
Intense cooperation with families
The provision of early intervention services is realised
in the following stages:
Initially, the ECI specialist provides the parents with
information about the child’s situation and condition
in friendly and understandable language. They are
also informed about the prospects of the child’s
development. For example: “Every child is born with
a different potential and it is difficult to make precise
forecasts, but when you love, support, and stimu-
late your child, they will progress.” Parents are also
informed about the availability of relevant services in
the community, if any. Often, however, there are no
other support services.
Assessment tools are used as an entry to the ser-
vice. One of these is a screening test for emotional
development called an ASQ-3 (Ages & Stages
Questionnaire) which evaluates a child’s development
compared to their age standard. It is a developmental
screening tool designed for use by early educators
and health care professionals. Another tool is the
ASQ-SE, which assesses emotional development and
is used mostly by parents in the home when a child
has not had a professional diagnosis.
Yet another tool is the Assessment, Evaluation,
and Programming System for Infants and Children
(AEPS) test. The purpose of the AEPS is to assist
professionals and parents/caregivers in identifying
and monitoring children’s developmentally appro-
priate educational targets and for planning individ-
ualized intervention. Moreover, regular re-testing is
conducted (in six-month intervals) with both tools
(ASQ and AEPS) to measure the child’s progress in
various areas.
The re-testing shows the achieved results against
the defined goals in the individual development plan.
All the information from these tests, medical documen-
tation, observations, other expert opinions, and the
resources of the family are taken into account, and an
individual development plan is developed together with
the parents. This plan includes goals and tasks within
a certain period, which is revised and amended at
three to six-month intervals. Importantly, the goals are
realistic and achievable in the everyday environment.
The ECI sessions are conducted in the child’s natural
environment – at home or at the playground – which is
why the services are mobile and are provided through
home visits. The purpose of the home visit is that the
ECI specialist can support and guide the family on
how to use available resources/objects at home for
stimulating the child’s development. In this way, the
development process is continuous and does not de-
pend on the presence of the specialist. All members
of the family are encouraged to participate. Parents
can become their child’s best therapists, since they
know the child best and are with the child for the
most time.
During each home visit, the specialist and parents
discuss the child’s progress, concerns, difficulties, and
everything that has happened since the previous visit.
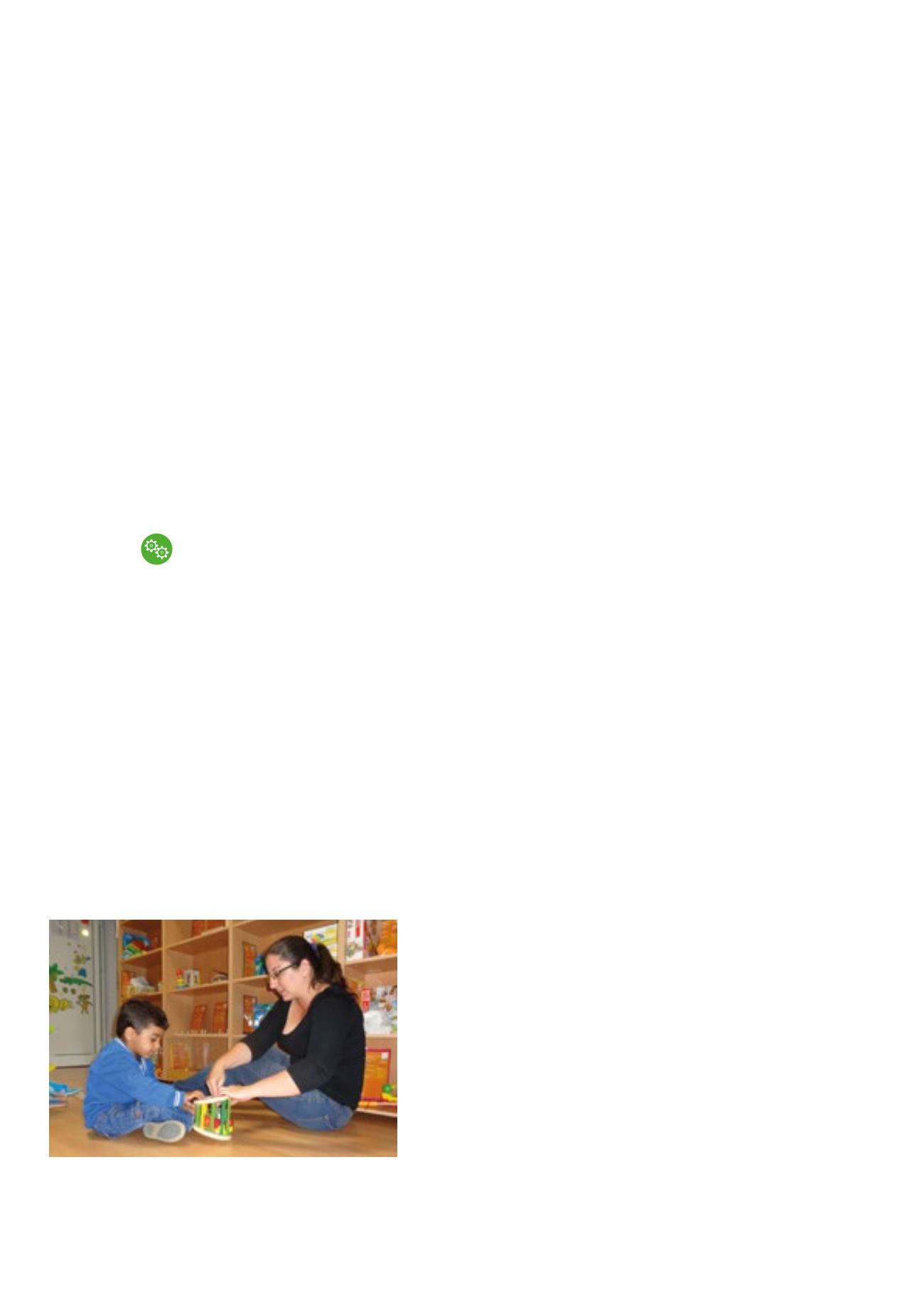
New activities or approaches might be suggested.
Each new activity is shown by the specialist and then
tried by the parent to make sure they will be able to
continue with it afterwards. This individual approach
is applied to each child and family, and the everyday
activities are adapted to the specific condition of the
child.
Each new activity is shown by the specialist and then
tried by the parent to make sure they will be able to
continue with it afterwards.
By integrating the early intervention
programme into the health and
social systems, the number
of abandoned children can be
significantly reduced